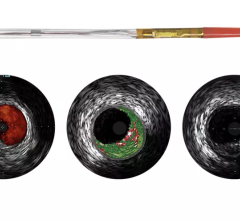
Volcano's Virtual Histology IVUS system showing plaque components defined by type.
September 29, 2009 – Volcano Corp. released imaging results from PROSPECT Trial, which demonstrated the progression of cardiovascular disease via precise, intravascular imaging, and the ability of Volcano's proprietary VH-IVUS technology to be used to classify lesions by plaque "type" per the PROSPECT protocol and to assess the risk of each plaque type to cause an event, or to remain stable out to three years.
PROSPECT (Providing Regional Observations to Study Predictors of Events in the Coronary Tree) results presented Sept. 24 at TCT 2009 include the landmark finding that angiographically mild lesions with certain morphologic features on grayscale and VH IVUS present with a three year cardiac event rate of 17 percent, versus other morphologies (indistinguishable by conventional angiograms) with three year event risks of less than 1 percent. The landmark 700 patient natural history study sponsored by Abbott and co-funded by Volcano
"For years, interventional cardiologists have been focused on using angiography to identify blockages and to restore flow. PROSPECT teaches us that looking at the angiographic severity of the blockage is not enough, and we must understand the type of disease present in the vessel wall," said Gregg Stone, M.D., of Columbia University Medical Center and principal investigator of PROSPECT. "With VH IVUS we can clearly see two things: one, that "mild" lesions on angiography are capable of progressing quickly into events for the patient: and two, events also take place in locations of severe disease that are often missed by angiography. Understanding the risk of each lesion type is paramount to minimizing the occurrence of these future events. Current practice using angiography guidance alone is insufficient in that regard."
PROSPECT is a first-of-its-kind multicenter, natural history study of acute coronary syndrome (ACS) patients. These patients underwent PCI to restore blood flow at baseline. Following the PCI procedure, an angiogram and a detailed IVUS image was captured in the three primary coronary arteries before the patient was sent home. If the patient had a subsequent event, they were readmitted, and again, an angiogram and IVUS imaging was performed. The core laboratory (Cardiovascular Research Foundation, New York) then matched the location of the secondary event to the initial IVUS images to determine which locations progressed, and which lesions remained stable. Patient follow-up continued for three years.
Volcano said angiography alone is not enough and more and more clinical data continues to support that conclusion. PROSPECT has shown that not all coronary disease is the same. The company said doctors cannot predict a patient's risk of having future cardiac events by looking at a 2D, black-and-white image of the arterial lumen. Available tools like IVUS and VH-IVUS that look at the quantity, location and type of disease and not just the narrowing of the vessel improve a doctor’s ability to determine the likelihood of a particular lesion type to cause an event. PROSPECT has shown the ability to use VH and grayscale IVUS to classify different lesion types per the PROSPECT definitions. The company said the trial highlights the potential of Volcano's VH-IVUS and the limitations of using angiography alone.
VH-IVUS uses advanced spectral analysis of the ultrasound signal to classify atherosclerotic disease into different plaque components. By using these four plaque components, the PROSPECT investigators grouped the baseline lesions into five distinct lesion types; fibrotic, fibro-calcific, pathological intimal thickening, thick-cap fibroatheroma and thin-cap fibroatheroma, in order of hypothesized risk.
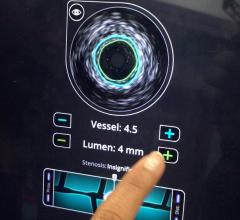
The PROSPECT event data demonstrates the measurements made using grayscale and VH-IVUS did have a statistically significant impact in determining the likelihood of a particular lesion type to cause an event. The highest risk PROSPECT plaque type being VH thin cap fibroatheromas with a minimum lumen area of less than or equal to 4 mm and a plaque burden greater than or equal to 70 percent. All three of these important parameters (each an independent predictor) when combined showed that the particular lesion imaged at baseline had a 17.2 percent chance of causing an event within three years. It is important to note that current practice of using angiography alone cannot measure plaque burden or the presence of VH-TCFAs, which were the two most significant predictors of lesion risk in the study. These measures can only be collected using Volcano's proprietary Eagle Eye Gold IVUS catheter not only visualizes and measures plaque burden but also collects signals for VH imaging allowing display of four plaque components.
Importantly, the absence of a fibroatheroma by PROSPECT definitions in imaged lesions was a strong predictor of lesion stability over three years as shown in the graph below. In lesions defined by PROSPECT having less than 10 percent necrotic core (red on VH-IVUS), the likelihood of that lesion progressing to an event over three year was negligible, independent of other grayscale and angiographic factors.
It is widely believed that a hazard ratio of greater than 2 is a clinically meaningful predictor of an event. You can see from the chart below that the hazard ratio for a PROSPECT defined VH-TCFA is 3.8 with a p-value of less than 0.0001 indicating a positive predictive value of causing an event that is statistically significant. The converse is true for PIT lesions, which have a hazard ratio of only 0.2, indicating low likelihood of causing an event, which is also statistically significant.
Volcano said VH-IVUS is a tool that allows physicians to further triage which lesions need to be stented, and which lesions can be treated with medical therapy. The negative predictive accuracy of VH-IVUS is very similar to fractional flow reserve (FFR) in its potential to reduce procedure costs by stenting only the patients and lesions that will benefit from that therapy.
For more information: www.volcanocorp.com

 September 18, 2025
September 18, 2025