
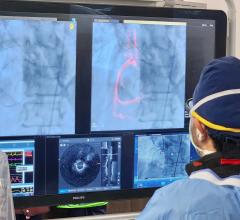
A comparison of a CT image of heavily calcified coronary arteries that appear to present a significant hemodynamic blockage and the corresponding FFR-CT showing the patient had adequate blood flow and does not need a diagnostic angiogram or intervention. Image courtesy of Kavitha Chinnaiyan, William Beaumont Hospital.
The use of non-invasive fractional flow reserve CT (FFR-CT) was the hottest topic discussed at the Society of Cardiovascular Computed Tomography (SCCT) 2018 meeting in July. The technology uses CT-derived FFR measurements for hemodynamic flow through the entire coronary tree, similar to invasive, catheter-based FFR pressure wire measurements. Clinical data and experience has been mounting with this technology for the past few years, and centers using it say it has been valuable to their hospitals and may offer a way to potentially reduce downstream costs.
FFR-CT has been discussed at SCCT for the last several years, but this year many sessions focused on how the technology is becoming mature enough to use routinely for real-world patient evaluations. The technology is gaining momentum and has recently racked up numerous reimbursement coverage decisions from the Centers for Medicare and Medicaid Services (CMS) and private insurance companies. This has mainly been driven by clinical evidence showing the technology can reduce the need for diagnostic angiograms or allow early discharge of patients who present in the emergency department (ED) where FFR-CT can definitively rule out severe ischemic heart disease.
FFR-CT has acted as a bridge at this traditionally diagnostic imaging-centered conference to incorporate the therapy side of interventional cardiology. Well known interventional cardiologist Morton Kern, M.D., has spoken on this technology at previous SCCT meetings, and this year interventional pioneer Patrick Serruys, M.D., Ph.D., Imperial College London, took center stage in a couple key sessions, declaring this technology is a major shift in cardiac diagnostics.
Serruys was the principal investigator of the SYNTAX III Trial, presented earlier this year as a late-breaking study at EuroPCR. He presented the trial again in sessions at SCCT. All 223 patients in the trial received a CT scan and were then split between two arms — one where treatment decisions were based on invasive angiography, and another where treatment decisions were based on CT and FFR-CT. The takeaway message from the trial was that interventional cardiologists using angiography and invasive FFR, and radiologists using FFR-CT, arrived at a 93 percent concurrence rate on measuring the severity of lesions.
“I got the CT scans the day I went into the cath lab with these patients. I know where the lesions are, I know the functional information on the lesion, and I even have the projection of the lesion in the LAD in the 3-D view, so I can convert that into the 2-D view in the cath lab. The planning value is extremely important,” Serruys explained. “It will be a paradigm shift."
While extremely helpful for interventional planning, Serruys sees the real future value of the technology as being able to detect and track disease very early. “I am thinking of young patients who have non-obstructive disease and using the multi-slice CT scan to see the progression of the disease.”
He said new PCSK9 inhibitor monoclonal antibody drugs now available can be used to regress heart disease and prevent the need for stents or bypass surgery if plaque formation can be reversed before reaching the stage of acute coronary syndrome. The use of statins can also be very helpful for disease prevention, but the problem is keeping the patient compliant over years and decades, which is where CT can play a new role.
“I think for the general practitioner, the cardiologist or the internist, if you can come to the patient with a colorful image and say, ‘Look, your anatomy is better, the position of the plaque is better and your physiology is better,’ that will be great incentive for these patients to continue their treatment,” Serruys explained.
This idea of using cardiac CT angiography (CCTA or CTA) for prevention has been echoed at SCCT for the past few years, where CT calcium scoring images can be used to help convince patients to go on, or stay on, statin therapy. Serruys said the new functional data provided by FFR-CT takes this a step further. The concept is that a picture is worth a thousand words and it is easier to communicate with patients about their disease, prevention paths and show them improvements caused by medications with CT imaging.
In the SYNTAX III Trial, Serruys said the CT and FFR-CT images and information were so good, that the cardiac surgeons came to him and said they no longer needed an invasive angiogram to confirm CT findings. They felt comfortable going directly to surgery. He said this has prompted a new trial that will look at the outcomes of CT-only guided cardiac bypass surgery.
Use of FFR-CT on a Daily Basis
Dozens of sessions at SCCT included many examples of how FFR-CT is being used in treatment decision-making at the several hospitals. Two of these presenters spoke with DAIC and confirmed the technology is ready for prime time. They claimed it has the potential to save money by reducing the need for additional tests, earlier discharge of chest pain patients who do not have a coronary occlusion, and the reduction or elimination of diagnostic angiograms.
Kavitha Chinnaiyan, M.D., FACC, FSCCT, associate professor, Oakland University, William Beaumont School of Medicine, Royal Oak, Mich., presented on Beaumont Hospital’s extensive use of FFR-CT. The center uses it as a rule-out test for chest pain patients presenting in the ED and to screen stable outpatients with suspected coronary disease.
“The strength of this technology is its ability in adjudicating patients who have intermediate stenosis on coronary CTA,” Chinnaiyan explained. "It is less of an issue if they have severe disease where we know what to do. But in the intermediate range, that is where we run into problems because we are unable to discern if that stenosis is leading to ischemia or not. CT angiography is an anatomic test, and we don’t get physiologic information. In the past, we would have to do another kind of test — perfusion testing, stress testing or invasive coronary angiography with invasive FFR.”
One issue with FFR-CT is that it requires exam datasets to be sent to the technology provider HeartFlow in California, because of the super-computing power needed to run the FFR-CT algorithms. A couple years ago, result turnaround times could be up to 12-24 hours. Today, Chinnaiyan said this has dropped significantly to five hours or less, so it can be used for ED patient diagnosis.
“We have seen, over time, a gradual decrease in the number of diagnostic caths,” she said. “This has happened gradually over the last three years of using the FFR-CT technology as all the cardiologists became more comfortable with using it. There is good cause for skepticism, but we have found that the correlations are pretty strong between invasive FFR and FFR-CT, so there are more believers now.”
She said FFR-CT will likely lead to changes in what insurance companies pay for because the technology has the potential to reduce downstream costs of extra testing, admissions and possible complications from catheterizations.
“The impact this technology has had on our institution’s practice of interventional cardiology has been significant,” Chinnaiyan said. “If you can get both anatomical and physiologic data with one test and avoid additional testing, then it would make a lot of sense for insurance providers to pay for this.”
Watch the interview with Chinnaiyan in the VIDEO: Using FFR-CT in Everyday Practice.
FFR-CT May Reduce Diagnostic Caths
“As an interventionalist, I really don’t like diagnostic catheterizations,” said Jeffrey Schussler, M.D., FACC, FSCAI, FSCCT, FACP, an interventional cardiologist at Baylor Scott White Heart and Vascular Hospital, Dallas. He spoke in a session about Baylor’s use of FFR-CT. “If I am going to have somebody in the lab and catheterize their heart, I really want to be able to do something to open up arteries. So, having some knowledge of what is going on in the heart prior to going in is very helpful. FFR-CT really gives us some insights into whether or not a blockage is physiologically important.”
He said 90 percent of the patients who get FFR-CT at Baylor Heart Hospital are usually very stable outpatients. This means scans are not usually time sensitive, so a delay in getting results back from Heartflow is not an issue. “We just need the answer to the question of whether these patients have coronary disease and is it bad enough to warrant invasive evaluation,” he said.
“In the past, these patients would have been given other tests for evaluation,” Schussler continued. “Stress testing has been used for years, but it is not that great. It is only about 80 percent sensitive and specific, so we are wrong about patients one in five times. A lot of people come in and get a stress test. It is negative. They go back out and they are still having chest pain. Prior to CT, they were all sent to the cath lab. With CT, when you really don’t think they have coronary disease, a negative CT makes it a one-and-done test. I think it has cut down on the number of people who would have gotten a heart cath or would have gotten a stress test, but now we just do one test and we don’t have to do any more diagnostics.”
Related FFR-CT Content:
Clinical Applications of FFR-CT
VIDEO: Early U.S. Experience With FFR-CT in Evaluating ED Chest Pain Presentation — Interview with Simon Dixon, M.D.
VIDEO: Implementation and the Science Behind FFR-CT — interview with Jame Min, M.D.
VIDEO: The Status FFR-CT Adoption in the United States
New Technology Supports CT as Prime Cardiac Imaging Modality

 May 05, 2023
May 05, 2023